
Below are the April Medical Staff Updates. As a reminder, all providers must complete the attestation at the bottom of this page by April 30.
Medical Leadership Message
 As Kaleida Health opens the second quarter of 2017, everyone is looking forward to the final stages of construction of the John R. Oishei Children’s Hospital and new beginnings at Conventus. The Oishei Children’s Hospital is on time, on budget and about 85 percent complete. Staff and physicians will begin on-site trainings and simulations in September in preparation for the move in early November. The team at Women & Children’s Hospital of Buffalo will begin mock moves of equipment and mock patients this month, conduct time studies, and begin to articulate the details of the move day.
As Kaleida Health opens the second quarter of 2017, everyone is looking forward to the final stages of construction of the John R. Oishei Children’s Hospital and new beginnings at Conventus. The Oishei Children’s Hospital is on time, on budget and about 85 percent complete. Staff and physicians will begin on-site trainings and simulations in September in preparation for the move in early November. The team at Women & Children’s Hospital of Buffalo will begin mock moves of equipment and mock patients this month, conduct time studies, and begin to articulate the details of the move day.
At Conventus, the Oishei Children’s Outpatient Center continues to welcome patients in a limited number of pediatric centers. Beginning this month, UBMD will begin seeing patients in many of their adult and pediatric outpatient offices on the fourth floor.
Reflecting upon the first quarter, there are opportunities to continue to improve our patients’ experiences. One of the key drivers of the patient experience is the interaction between our teams and our patients. Overall, 95 percent of patients report their physicians “usually” or “always” communicate well. However, in the first quarter, there was a decrease in the percent of patients who report physicians “always” treat them with courtesy, listen carefully and explain things in a way they understand. Tactics that are proven to improve communication include:
- Review the patient’s chart and work-up to date prior to your initial encounter, and summarize your understanding of their history and plan
- Ask the patient to explain their understanding of their diagnosis and plan
- Incorporate the patient’s goals into their treatment plan
- Summarize the plan on the patient’s communication board
Consistent, engaging communication from all physicians drives patient understanding, compliance and outcomes. Additional tools and communication tactics will be available on Talent Management for all physicians.
Thank you for your continued commitment to our patients and their families!
David Hughes, MD, MPH
Chief Medical Officer
Kaleida Health
Kenneth Snyder, MD, PhD
Vice President, Physician Quality
Kaleida Health
Colin McMahon, MD
Chief Medical Officer
Buffalo General Medical Center/Gates Vascular Institute
David Pierce, MD, FACEP
Chief Medical Officer
Millard Fillmore Suburban Hospital and DeGraff Memorial Hospital
Stephen Turkovich, MD
Chief Medical Officer
Women & Children’s Hospital of Buffalo
Message from the President of the Medical/Dental Staff
 As I write this, the Republican leadership of the House has just pulled the American Health Care Act (AHCA), knowing it would not pass a vote. If it had passed, the AHCA would have “take[n] away health insurance from an estimated 24 million people and raise[d] costs for many older Americans. It would [have] channel[ed] the savings into large tax cuts for the affluent…It would [have] also substantially cut Medicaid, a program that insures poor people as well as many elderly and disabled who aren’t poor” (David Leonhardt, New York Times, March 23, 2017 https://nyti.ms/2mU3jIC).
As I write this, the Republican leadership of the House has just pulled the American Health Care Act (AHCA), knowing it would not pass a vote. If it had passed, the AHCA would have “take[n] away health insurance from an estimated 24 million people and raise[d] costs for many older Americans. It would [have] channel[ed] the savings into large tax cuts for the affluent…It would [have] also substantially cut Medicaid, a program that insures poor people as well as many elderly and disabled who aren’t poor” (David Leonhardt, New York Times, March 23, 2017 https://nyti.ms/2mU3jIC).
This ill-considered bill was opposed by every major healthcare association, including the American Academy of Pediatrics, the American Medical Association and the American Hospital Association. It deserved the opposition.
As healthcare professionals, it is our duty to provide the highest quality care to our patients. It is also our duty to ensure that our patients have access to our care. A critical part of access is high-quality insurance. It is well documented that insurance status is tied to health status: good insurance improves health. As an example, a recent study comparing cystic fibrosis survival in the United States and Canada demonstrated that survival was much better in Canada, a difference that was almost entirely explained by the better insurance coverage in Canada (Ann Intern Med. Published online March 14, 2017. doi:10.7326/M16-0858).
Although the AHCA was deservedly defeated, this is likely to be but one battle in a long war. The President and his administration have made it clear that they do not have an interest in providing healthcare insurance, especially to the most vulnerable. Their budget, by largely defunding the NIH, also clearly demonstrates they do not value healthcare research.
As healthcare providers, we must be vigilant against these kinds of attacks. I urge you to remain informed and to call (which is much more effective than email or online petitions) your senators and representatives to express your opinions.
Peter Winkelstein, MD, MS, MBA, FAAP
Medical/Dental Staff President
Kaleida Health

Medical/Dental Staff Semiannual Meeting on April 27
All Kaleida Health and ECMC physicians and advanced practice providers are invited to the Medical/Dental Staff Semiannual Meeting on Thursday, April 27, 2017, at Templeton Landing in Buffalo.
Cocktails and hors d'oeuvres begin at 5:45 p.m.; the business meeting and dinner will begin at 6:30 p.m.
Guest speaker David Rich, executive vice president, government affairs, communications, and public policy, Greater New York Hospital Association, will discuss the current political climate and its impact on health care. CME credit will be available.
Due to limited space, this event is first-come, first-served, and RSVP is required by Friday, April 14, 2017. If you are attending, please be sure to add the meeting to your own calendar as there will not be an invitation sent via Microsoft Outlook.
Visit the Survey Monkey link to RSVP and select your meal choice. For questions, call the Kaleida Health Medical Staff Office at 859-5501.
Quality Update at Kaleida Health
Monthly Webinar: DNV GL Survey Preparedness
This month's webinar features Kristen Bies, director of accreditation readiness, discussing the upcoming DNV GL survey. For questions, please email kbies@kaleidahealth.org or call 716-859-8520.
Click HERE to watch the webinar.
Hand Hygiene – Emergency Call-to-Action
 Kaleida Health staff recently participated in an emergency call-to-action to improve hand hygiene and reduce hospital acquired infections (HAIs). Please remember, if you cross the plane of the door, regardless if you touch anything, you must perform hand hygiene.
Kaleida Health staff recently participated in an emergency call-to-action to improve hand hygiene and reduce hospital acquired infections (HAIs). Please remember, if you cross the plane of the door, regardless if you touch anything, you must perform hand hygiene.
A best-practice hand hygiene product, Purell, has been rolled out at all the hospital sites and in our long-term care facilities. Touchless dispensers are now available in more convenient locations to improve use.
If you are approached by a care team member to wash your hands, say "thank you" and perform hand hygiene. We are all working together to reduce HAIs and ensure safe, quality care for our patients.
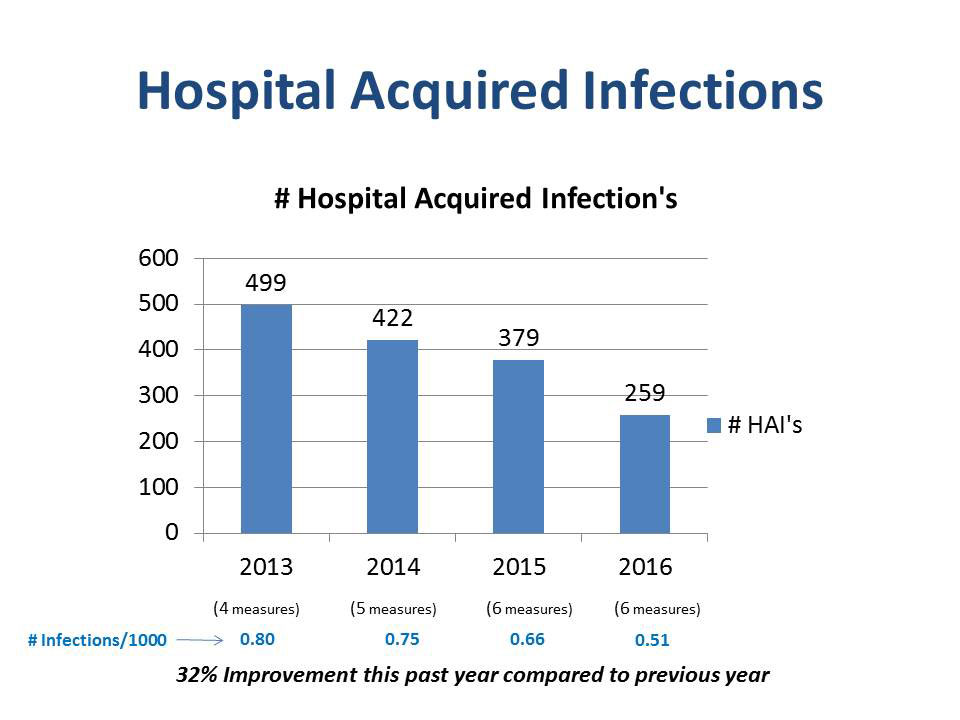
Hospital Acquired Infections
 click to enlarge
click to enlargeKaleida Health has seen a dramatic decrease in hospital acquired infections (HAIs). Teams focused on the top 5 HAIs reviewed evidence-based practices to revise current policies and procedures and standardize care across the system. Each infection is investigated to determine the apparent cause, allowing the teams to trend issues and put action plans in place. Quick wins from each team include:
- CAUTI – Appropriateness of culture ordering; daily assessment to remove catheter
- CLABSI – Implementation of the curos cap, reducing contaminated blood cultures and chlorhexidine-containing dressings
- Colon SSIs – Implementation of the colon bundle (antimicrobial prophylaxis, glucose control, normothermia, skin prep, perioperative oxygenation and clean standardized fascia close)
-
C. diff and MRSA – Hand hygiene, antibiotic stewardship, environmental cleanliness and investigations of clusters of infections for root cause
See below to review Kaleida Health’s progress in reducing HAIs since 2013.
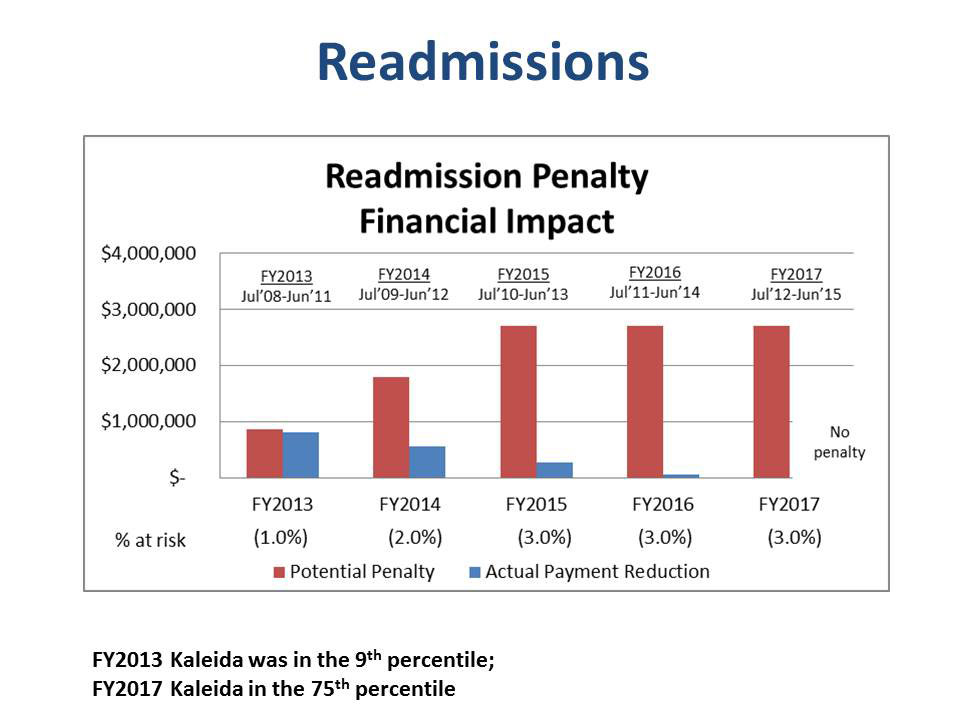
Readmissions
The Readmission Reduction Program at-risk started at one percent of the diagnosis-related groups (DRG) base payment in Fiscal Year (FY) 2013 and increased to three percent by FY2015 where it remains. Readmissions are measured in acute myocardial infarction (AMI), heart failure, pneumonia, coronary artery bypass graph, and total hip/total knee arthroplasty.
 click to enlarge
click to enlarge
Kaleida Health is the only local hospital that did not receive a penalty for FY2017. The FY2017 readmission results reflect performance from July 1, 2012-June 30, 2015.
Kaleida Health is seeing readmissions trending up and recently reconvened the readmissions team to evaluate best-practices to reduce readmissions and develop an action plan for improvement.
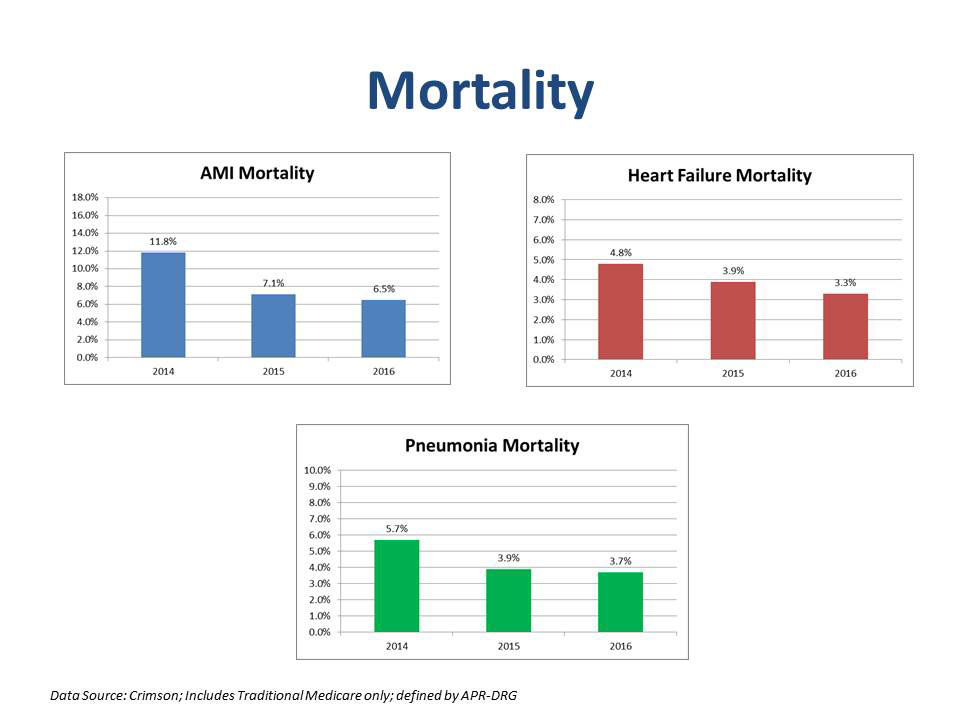
Mortality Rates
 click to enlarge
click to enlargeMortality rates in the three primary diagnosis categories of acute myocardial infarction (AMI), heart failure and pneumonia have all decreased in the past few years. The incorporation of evidence-based medicine has greatly contributed to the mortality reduction, as well as multidisciplinary rounds and rapid response teams. Kaleida Health is currently evaluating palliative care services to improve the quality of life and care of adults with serious illness.
Finance Update
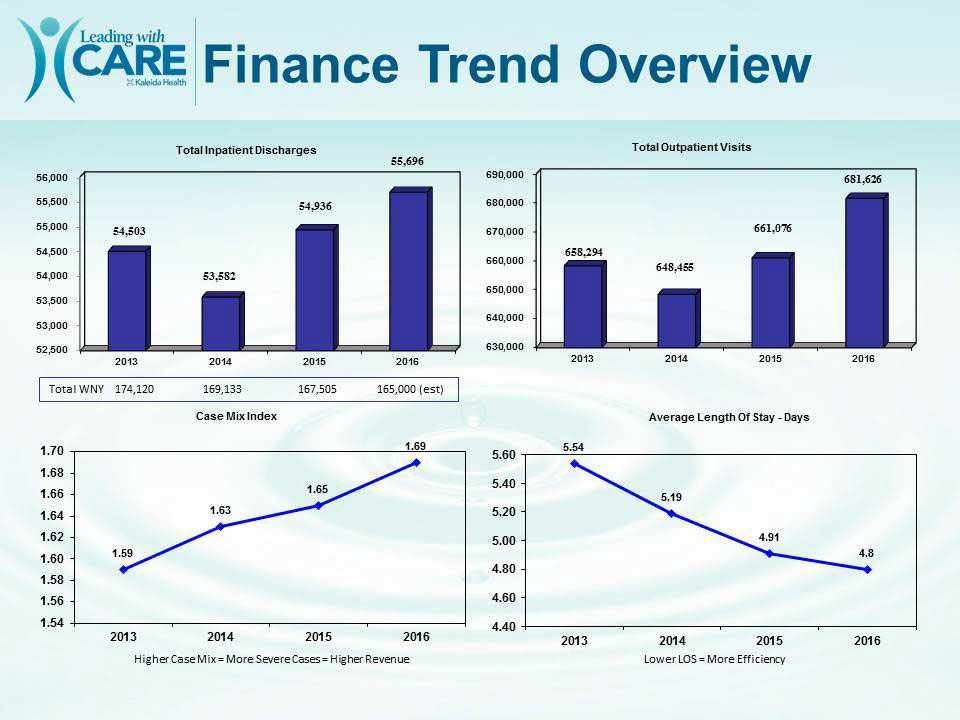 click to enlarge
click to enlarge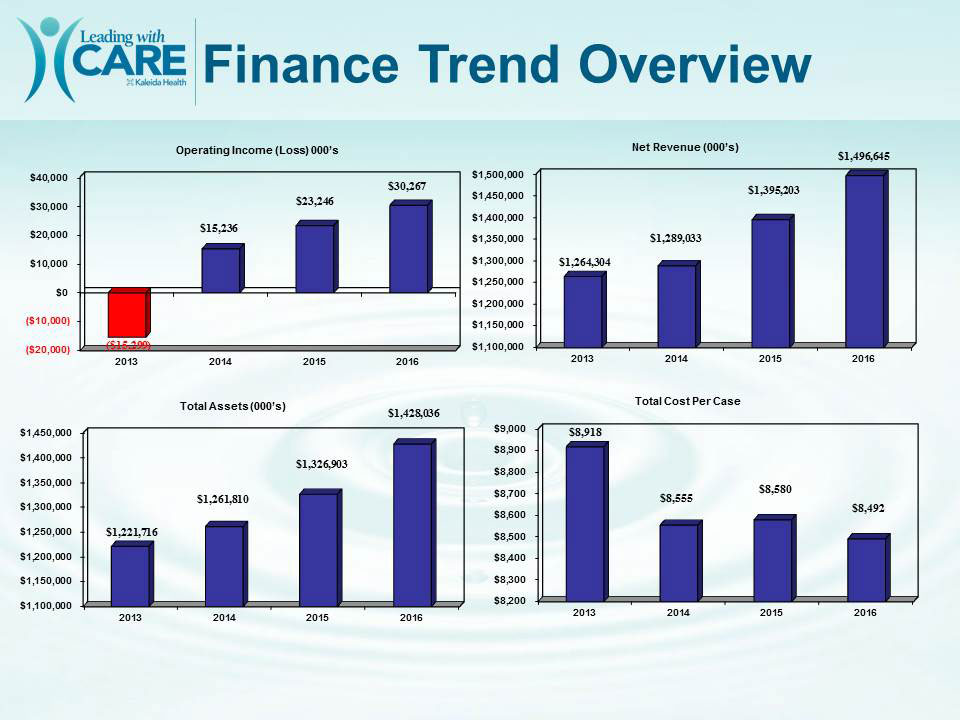 click to enlarge
click to enlargeThe organization continues to head in the right direction financially. Kaleida Health's total net assets are up, and our bottom line continues to increase. Please see to the right for more details and share this information with your staff.
Medication Reconciliation
There is a heightened sense of urgency related to the accuracy and completeness of discharge medication documentation from Kaleida Health to the next level of care.
The provider may begin the discharge process in the Electronic Medical Record (EMR), but may not complete it at a later point in time prior to the discharge. The discharge order may be entered prior to the completion of the discharge summary. There are 3 steps for the workflow in the EMR in order to have an updated final list of medications for the discharge summary:
- Sign the discharge summary after discharge medication reconciliation is complete
- Refresh the discharge medications component of the discharge summary after completing discharge medication reconciliation
- Enter discharge order after you have signed the discharge summary
New York State Electronic Death Registration System
Legislation enacted in September 2013 created an addendum to Public Health Law 4148, which authorized the Department of Health to develop, implement and maintain an Electronic Death Registration System (EDRS) for the purposes of electronically completing, filing and maintaining death certificates in New York State.Beginning Monday, March 20, 2017, death certificates must be filed electronically in the EDRS, an application within the New York State Health Commerce System (HCS), when the death occurs at an acute care site or long-term care facility.
Instructions for Licensed Practitioners
- Providers who are registered with New York State to prescribe medications (providers who have an I-STOP account) already have access to the HCS. Please send your user ID to Pamela Birke at pbirke@kaleidahealth.org. Pamela will assign the EDRS application to your account.
- Providers who are not registered with New York State or do not have access to the HCS should follow these instructions:
- Visit https://commerce.health.state.ny.us/public/hcs_login.html (This link is available under KaleidaScope – Applications – General Applications – “HCS – NYS Dept of Health, Health...”)
- Select “Lic. Med. Prof.” in the bottom left corner
- To apply, you will need a New York State driver’s license or New York State non-driver picture ID as well as a New York State Education Department registered medical professional license
- Fill out application
- Agree to terms
- Create a new password
- Send your user ID to Pamela Birke at pbirke@kaleidahealth.org
If you need assistance, please visit your site’s Health Information Management Department or Medical Records.
For additional information or training, visit https://www.health.ny.gov/vital_records/edrs/.Medicare Outpatient Observation Notice (MOON) Act
The Medicare Outpatient Observation Notice (MOON) Act is the mandatory notification to all Medicare beneficiaries that “they are a hospital outpatient, receiving observation services.” Effective March 8, 2017, the notification must be given by the provider (MD, PA, NP) both verbally and in writing within 24 hours and no longer than 36 hours, “that they require a period of observation to evaluate their condition.”
The form is printed at the time of patient registration and is placed in the chart for completion. This notification is given to ALL patients at the time of registration in the Emergency Department by the registrar notifying patients that they are being placed in observation to further evaluate their clinical condition. If the patient refuses to sign the notice, the provider should document “patient refused” along with date and time.
The MOON Act does not replace form KH01425 – OBESERVATION NOTIFICATION.
The notification defines:
- Medicare Part B coverage
- Copayments
- Skilled Nursing Facility – medical necessity
- Provides 1-800-MEDICARE contacts should the patient wish to reach out to CMS
Applicable Policies:
- PT.8 Your Rights as a Hospital Patient
- MED.39 Outpatient Observation Services
- PM.19 CMS Important Discharge Notice
- PM.3 Complying with Provisions of the Care Act
Involved Personnel:
- Physicians, physician assistants, nurse practitioners, nurses
- Hospital Utilization and Discharge Planning are available to answer any questions or concerns
New York State Pain Course – A Mandate for All Prescribers
New York has mandated that by July 1, 2017, every person licensed under Title Eight of the Education Law (physicians and other health professionals) and registered under the Federal Controlled Substances Act and in possession of a DEA registration number, and every medical resident who is prescribing under a facility DEA registration number shall complete three hours of course work or training in eight clinical areas related to pain management, palliative care, and addiction as approved by the Department of Health. This  click to enlarge
click to enlarge
The NY Chapter ACP in conjunction with Boston University School of Medicine has developed a 3-hour online CME Course that is also eligible for 3 ABIM MOC points. By completing this online course and post test questions, all prescribers will satisfy the requirements and obtain the necessary certificates as mandated by Chapter 71 of the Laws of 2016.
Specific elements contained within the 3-hour educational course:
- State and Federal laws on the prescribing of controlled substances
- Pain Management
- Appropriate Prescribing
- Managing Acute Pain
- Palliative Medicine
- Prevention/Screening/Signs of Addiction
- Responses to Abuse and Addiction
- End of Life Care
To access full course details and instructions, visit http://www.nyacp.org/i4a/pages/index.cfm?pageid=3831.
Doximity – Vote for Kaleida Health on Surveys

Physicians who are members of Doximity, the largest professional network for U.S. physicians, are encouraged to help promote Kaleida Health when surveyed by Doximity. Surveys are regularly sent to Doximity users, including U.S. News & World Report’s annual Hospital Rankings. One of the measures in the Hospital Rankings is “Reputation with Specialist,” which accounts for nearly 30 percent of the overall score in each specialty. When surveyed by Doximity, please list Kaleida Health as a top hospital for a particular specialty, which will ultimately lead to our specialties being ranked in U.S. News & World Report.
Kaleida Health Implementing Plain Language Emergency Code
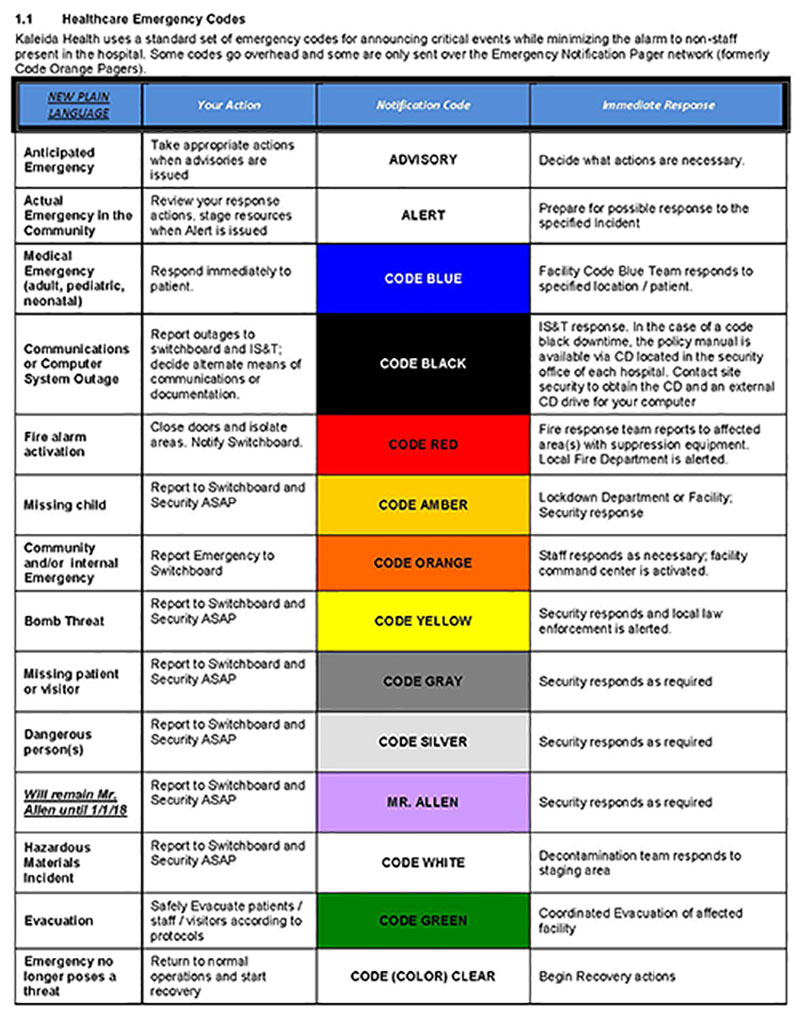 click to enlarge
click to enlarge
In an effort to promote safe, high-quality care, Kaleida Health is implementing plain language emergency codes. Plain language is communication the audience can understand the first time they hear it. People know what actions are required based on the information they receive.
Along with the move to plain language codes, Kaleida Health will be utilizing silent notification options more often to reduce noise and provide a quieter environment for patients to rest and heal.
Historically, hospital emergency codes were assigned a color to convey essential information quickly and with minimal misunderstanding to staff, while preventing stress and panic among hospital visitors.
However, there is significant variation of color codes across organizations, which causes confusion among healthcare providers. In addition, patients and visitors want more transparency and have shared feedback that color codes actually increased their stress level.
The recommendation to adopt standardized, plain language emergency codes was developed by experts from hospitals across the nation and is based on scholarly literature, research and national guidelines.
As Kaleida Health transitions to plain language emergency codes, both the color code and plain language code will be announced beginning April 1, 2017 with formal rollout of plain language on May 1, 2017.
Clinical Research: Lung and Cystic Fibrosis Center at Women & Children’s Hospital of Buffalo

The Lung and Cystic Fibrosis Center at Women & Children’s Hospital of Buffalo is a participating center of the Therapeutics Development Network (TDN). The TDN is composed of 82 sites across the country and through this network we are able to be at the forefront of CF research.
CF affects more than 70,000 people worldwide; it is the most common fatal genetic disease but still an orphan disease. CF is caused by a defect in the gene encoding the CF transmembrane conductance regulator (CFTR), an ion channel that regulates the flow of chloride in epithelia of the lungs, pancreas, intestines, reproductive organs, and sweat glands. Decreased CFTR activity leads to excessively thick mucus. In the lungs, this results in obstruction, inflammation and bronchiectasis, ultimately resulting in respiratory failure and death. Despite progress in the treatment of CF, the median predicted survival is 40 years. More effective treatments are needed.
At Women & Children’s Hospital of Buffalo, we participate in over 15 CF research studies. We have participated in studies of ground-breaking compounds that correct the CFTR protein, leading to the approval of OrkambiTM (Lumacaftor/Ivacaftor) and KalydecoTM (Ivacaftor). Our studies include observational and randomized controlled studies of the new CFTR modulator therapies. Other studies we perform include studies on growth and nutrition, antibiotics, adherence to treatment and mental health in CF; together with the department of Psychiatry, we are leaders in developing depression and anxiety screening processes for CF patients.
Please contact the CF Research Team at (716) 878-7524 if you would like more information.
Medical Staff Attestation - April 2017
By submitting this attestation, I confirm that as a member of the medical staff I have read and understand the information included in this email from Kaleida Health in accordance with Kaleida Health policy MED.41 as approved by the Medical Executive Committee.
| Fields marked with an asterisk (*) are required. |
|
|